
The Developmental Station is one of the more varied stations in the examination. From an examiner’s point of view, they want to see that you have a logical system for assessment, that you can adapt this to the child you have been given, and that you can put it together logically and come to a conclusion.
To demonstrate additional skill, candidates may be able to integrate the developmental findings with other signs that have been seen during the course of the examination.
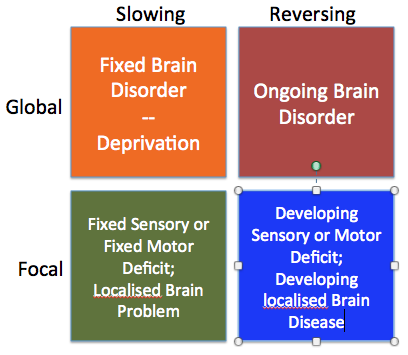
This section of the website features common sorts of developmental cases that turn up in the station. In clinical practise, children presenting with developmental issues should be divided into those with slow development and those with regression. For both slow and regression, some children with have a problem in all developmental scales (global), and other where one scale dominates the others (focal). Those with regression have an active ongoing disorder (brain tumour, hydrocephalus, deteriorating muscles or vision for instance) and are extremely unlikely to be in the MRCPCH. However in your clinical work, mis-managing this group can be devastating. Those with global delay or delay affecting a specific scale are much more likely to be there.
This diagram shows this with a few example conditions.

Global delay
Here there is delayed development in all scales – gross & fine motor, hearing/speech/language and social. Candidates should identify the developmental age in each scale, using the guide on this website or another suitable approach. It may be that the brain growth is also slow, leading to microcephaly. There may be typical facial or other features suggesting the underlying cause of the disorder. Remember to do what the examiner tells you. In the development station, you need to look at development, not dysmorphology, as that is where the marks are.
Common causes of Slowing/Delay
Global Delay
Down syndrome or another genetic disorder is most likely – these are stable patients, well known to the examination centre and the examiners. They will probably have Global Delay. Look for small stature, facial features, the ears, scars suggesting cardiac surgery. Children with Down syndrome are hypotonic, with a hypotonic posture. They often have serous otitis media in association, which may lead to focal delay in addtion in the hearing/speech/language scale.
Children who have suffered moderate or severe Hypoxic Ischaemic Encephalopathy are likely to have global developmental delay. Some scales are affected more than others, and there are likely to be associated with other neurological findings, such as a diplegia, a hemiplegia, hypertonia and contractures. This will depend on the particular areas of the brain affected.
Focal delay predominantly affecting one scale
If a condition is causing delay in one scale, it is important not just to measure this, but also to look for how the impairment in that scale is spilling over into other areas of development. For instance, gross motor delay may prevent development of hand/eye coordination; and hearing problems can lead to delay in social development.
Affecting hearing/speech/language scale
Most children with hearing/speech problems do not have an underlying syndrome or dysmorphic features. Common causes include serous otitis media (glue ear), antibiotic related deafness and deafness related to prematurity. Look for scars on the back of hands, features of chronic lung disease and a hearing aid. Some children may be managed with a cochlear implant.
Some children with problems in hearing have a more extensive ear malformation. Goldenhar syndrome is an example. Look carefully for tags in front of the ear and the shape of the ear.
Affecting vision and fine motor scale
Here it is important to look both at the eyes and the hand function. Although eye milestones are usually accomplished by 6 weeks (fixing and following), further problems in development in this scale are typically around the performance of what the hands are able to do. Candidates should consider looking specifically for visual acuity, squint, and eye movements if it is likely that there is a visual explanation of the fine motor delay.
Retinobalstoma will have been managed if a child comes to the clinical examination. Most but not all cases are unilateral and will have a glass eye. These usually do not move as well as the normal eye.
Retinopathy of prematurity is often also accompanied by a squint. Look for other features associated with prematurity.
Children with myopia or hypermetropia will usually have had their visual defect corrected by the time ofe the exam. Without glasses they will have fine motor problems if the problem is severe enough.
Affecting gross motor scale
This is likely to be the commonest single scale defect. As this is a developmental station attention should be paid to the developmental performance rather than the neurological defect. Candidates should be able to examine this at least to the age of 5. Candidates may have an opportunity to show other signs such as -plegias, tone abnormalities or increased or depressed reflexes.
Spina bifida will mainly affect lower limbs leading to an upper motor neurone pattern of neurological abnormality. Functional from a development point of view there may be social delay with impaired bladder or towel function. Look for scars on the back and evidence of operations on the abdomen (ACE For instance).
Affecting social scale
Autism spectrum disorder is typically noticed first in infancy. The child develops some social awareness but continues to fall behind normal peers as he or she develops. Look for stereotypic behavious and poor speech.
Fragile X affects only boys and of these 50% also have autism features. There are some characteristic morphological changes including long facies and protruding ears.
Common Causes of Regression
Candidates are unlikely to see children with features of regression, as most are caused by ongoing organic disease (see diagram above), which needs to be urgently addressed. There are some examples where this is not possible and so these children may appear in the exam.
Duchenne muscular dystrophy only affects boys, although there are dystrophies such as Becker that affect both sexes. This disorder causes progressive developmental regression. Test for proximal weakness with tests such as shoulder shrugging and asking to patient to stand from a squatting position.
Spinal muscular atrophy has three types, and it is unlikely that the more severe type I will be in the exam. Type I I as with all gross motor problems affects proximal and truncal power. There is a progressive loss of power that develops in early and mid childhood.
Children with progressive and untreatable blindness may also be brought to the exam. This would most often be caused by retinitis pigmentosa. Offer to test eye movements, acuity and fundoscopy.

Wonderful and practical to start with as it is written in an easy and understandable language.