
1. On approaching a child:
Around room Oxygen tank (pulm HT); Saturation monitor
View from Distance
- Nutritional status: ‘I would like to plot his height and weight on a growth chart’
- Work of breathing: Respiratory rate, recessions
- Cyanosis
- Dysmorphism – top 3 syndromes: Down’s Williams, Digeorge
- Other possible syndromes related to CVS: Turner’s , Noonan’s
2. Fingers:
- Clubbing
- Peripheral cyanosis
- Splinter haemorrhages
- Capillary refill
Hands:
- Janeway lesion
- Osler nodes
- Tuberous and tendon xanthomas of familial hypercholesterolaemia
Bony abnormalities: Absent Radii (VACTERYL Syndrome)
Absent Thumb (Holt-Oram Syndrome)
Pulse- Radial and brachial
HR (Count, rhythm, character) – count over 6 sec X10
Blood pressure
Radio-radial delay
Radio-femoral delay
Note: if cannot feel pulses – say ‘pulses are difficult to feel’
3. Face
Eyes: Sclera – Jaundice ( Congestive cardiac failure à Hepatic congestion)
Conjunctive – Pallor (Anaemia)
Face: Mitral flush / malar flush
Polycythaemia (Cyanotic heart disease à Increased haematocrit)
Tongue: Central cyanosis ( Right to left shunt/ Inadequate oxygenation in lungs)
Lips/oral mucosa: Pallor
Teeth: Dental Caries
Palate: High arch palate (Marfan’s)
Conjunctival injection and gum hypertrophy = chronic cyanosis
4. Neck:
JVP : Only in older children: Right heart failure, fluid overload)
Suprasternal notch : thrill in aortic stenosis
5. Praecordium
Inspection:
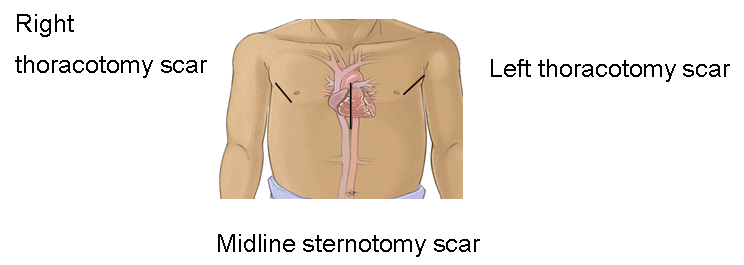
1. Scars: Back scars (link – pictures)
Front scars (link)
– See notes in blue for more information on scars
2. Visible pulsations (hyperdynamic apex beat)
3. Chest wall deformity
– Anterior bulge chest (cardiomegaly)
– Harrison sulcus (Increased pulmonary blood flow / asthma)
– Asymmetry
4. Respiratory rate
Scars:
|
Right thoracotomy scar |
|
Midline sternotomy scar |
|
Left thoracotomy scar |
Chest drain scars
Mediastinal drains
Chest wall pacemaker
Messy median sternostomy scars If no murmurs: differential includes hypoplastic leftheart syndrome due to Norwood 1 , 2, 3 .
Scars for Tetralogy of Fallot
Left or right thoracotomy scars in association with pulse on corresponding side
If bilateral thoracotomy scars — failure of one shunt and the need for second shunt procedure
Central sternotomy scar indicates definitive repair carried out – Childmay not be cyanosed , but may still have right ventricular outflow stenosis
Notes on Cardiac Procedures
1 . Repair : VSD , ASD , Tetralogy of Fallot repair
2 . Palliative:
A. Temporary:
BT shunt( to allow for pulmonary blood flow, encourage deviation ofpulmonary tree )
PA banding ( prevent overloading of thepulmonary circulation pending repair of large VSD )
Atrial septostomy ( transposition of great arteries )
Palpation
1. Apex Beat (Use both hands to feel both sides)
a) Site
Displaced to left: Cardiomegaly, pectus excavatum, scoliosis
Displaced to right: Congenital dextrocardia (feel for liver- Kartagener syndrome),
Left diaphragmatic hernia,
Collapsed lung on right,
Left pleural effusion,
Left pneumothorax
b) Character: Sustained
Forceful (LVH)
Thrusting : Volume overload (Large stroke volume ventricle in mitral/aortic incompetence, or left to right shunt)
2. Left parasternal heave à Right IVH / RV outflow tract obstruction
3. Thrills:
Thumb palpate at suprasternal notch for thrills at the same time
Lower left sternal edge: VSD
Upper left sternal edge: Pulmonary stenosis
Image source: http://www.childrenshospital.org/health-topics/procedures/heart-transplant
http://en.wikipedia.org/wiki/Hand
Auscultation:
Auscultate areas:
1.Mitral area (Apex area) to Tricuspid area (LLSE) to Pulmonary area (LUSE) to Aortic area (RUSE)
2. Also auscultate- Axillary area (if there is murmur at Apex or LUSE)
– Back (If there is murmur at LUSE)
– Neck (if there is murmur at RUSE)
3. Base of lungs for inspiratory crepitation in cardiac failure
|
ULSE:
Ejection systolic: Pulmonary stenosis ASD Innocent murmur |
|
RUSE:
Ejection systolic: Aortic stenosis Continuous: Rt BT shunt Venous hum |
|
Apex: Pansystolic: Mitral regurgitation VSD
Late systolic: Mitral Valve Prolapse Ejection Systolic: Aortic stenosis Mid-diastolic: Mitral stenosis |
|
LLSE: Pansystolic: Tricuspid regurgitation VSD Diastolic: Tricuspid stenosis Aortic regurgitation Still’s murmur |
|
Back: Systolic: coarctation (between scapulae), peripheral pulmonary stenosis Continuous: PDA |
|
5 types of normal murmur:
Innocent murmur do not radiate Pulmonary stenosis murmur radiate to the back and axilla Mitral regurgitation radiates to left axilla
To differentiate aortic stenosis from pulmonary stenosis: Murmurs louds in expiration à Left heart disease à Aortic stenosis Murmurs loudest in inspiration à Right heart disease à Pulmonary stenosis |
If there is a murmur, describe by:
– Systolic / diastolic murmur
– Site
– Loudness (Grade 1-6)
– Radiation
– Character: harsh, blowing, high-pitched, low-pitched
Anything else?
I would like to complete my cardiovascular examination by:
- Feeling for hepatomegaly
- Feeling for femoral pulses and looking for scars on inguinal area for cardiac catheterisation/ arterial lines
- Measure blood pressure and oxygen saturation (if not mentioned earlier )
- Measure height and weight and plot on growth chart appropriate for age and size
- Feeling for peripheral and sacral oedema
- Auscultate lung bases (if not done earlier)
Conclusions:
Don’t panic. Speak sense
When you present: Rather than describing your entire examination in detail, please present the salient points:
- Cyanosis/Pink
- Stable/not in respiratory distress
- Clubbing
- Scars
- Heart sounds I + II + murmur (grade)
Example of presentation:
I examined Peter, a 7-year-old boy who looks well-grown for his age and I would like to plot his height and weight on a growth chart.
He is pink and not in respiratory distress. There are no dysmorphic features or finger clubbing. There are no scars on his chest. There is a palpable thrill at his suprasternal notch. He has a grade 3/6 ejection systolic murmur at right upper sternal edge radiating to carotid area.
He has left ventricular outflow obstruction such as aortic stenosis.
Author: Dr. Huey Miin Lee, 2013

Well done. It is a really helpful & probably first of its kind to help out trainees to pass MRCPCH clinical exam. It would be more helpful if you help us with more videos especially communication scenarios & presentation of clinical cases to examiners.
Thank you.
thanks thanks thanks for this great job…
thanks again..
Presence of thrills means the murmur is grade 4/6
Thanks for the above description which is very helpful in the clinical exam
Great job !
I thank you very much for this very useful and brilliant site materials..
It is mentioned up that diaphragmatic hernia repair will result in a right thoracotomy scar but isn’t that it results in left thoracotomy scar most commonly?? (right sided are very rare).
thanx very much ….
very helpful&simplified
hoping for more videos in all branches showing more clinical case examinations joined with the discussion
thanks.very brilliant and very helpful
Very helpful. ..Thank u alot
it’s good teaching work,thank you a lot!!!
Thanks a lot
Very Useful information …Thanks .
Mnemonic suggestion
Left heart disease murmurs loud in expiration (AS)…E for E
Right heart disease murmur loud in inspiration (PS)…I for I
Thank you very much. It seems simple and perfect.
thank u very much! It was very informative and helpful. Well done!
Great effort .. well done …
I find it so helpful…
thanx alot ..
i also found a detailed lecture of this at https://www.youtube.com/watch?v=1G93LC9BlOc